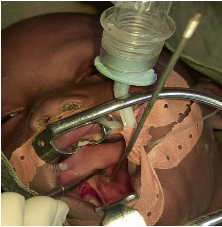
Introduction: Pharyngeal foreign bodies, particularly in oropharyngeal locations, should raise concerns about the presence of an associated wound. They constitute a common pathology. Their diagnosis is most often easy, but difficult in the case of an unknown foreign body. We report a foreign body embedded in the lateral wall of the oropharynx which required emergency tonsillectomy. Observation: This is a 6-year-old child received urgently at the Nianankoro Fomba Hospital in Ségou 6 hours after the introduction of the foreign body (wheel spoke) into the tonsillar compartment. On admission to the ENT and head and neck surgery department, the child's general condition was poor, consciousness remained and the conjunctivas were normal-colored. On oropharyngeal examination, we note a sharp metallic foreign body measuring 30 cm and 2 mm in diameter located at the level of the posterior fold of the right amygdala. Furthermore, there is hypersialorrhea with blood streaking. Faced with the failure of an extraction attempt; we decided to take him to the operating room after a minimum assessment. The immediate postoperative course was unremarkable. The evolution was very favorable on the 10th day of the intervention. Conclusion: Pharyngeal foreign bodies constitute a vital emergency due to their appearance or location. Their management requires rapid intervention with suitable equipment. Prevention remains the best solution.
| Published in | International Journal of Otorhinolaryngology (Volume 10, Issue 2) |
| DOI | 10.11648/j.ijo.20241002.12 |
| Page(s) | 54-57 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Foreign Body, Emergency, Tonsillectomy
ENT | Ear Nose Throat |
GA | General Anesthesia |
| [1] | Hervé S, Portier F, Chapot R, Guichard JP, Wassef M, Tran Ba Huy P et Herman P. Fibrome nasopharyngien. Encycl Méd Chir (Editions Scientifiques et Médicales Elsevier SAS, Paris, tous droits réservés), 20-585-A-10, 2001, 14 p. |
| [2] | Higgins GL, Meredith JT. Internal carotid artery thrombosis following penetrating trauma of the soft palate injuries: an injury of youth. J Fam Pract 1991; 32: 316-22. |
| [3] | BertrandV, Besson-Leaud L, Herve JF, Joubert C, Menager C, Yazici B, et al. Vascular damage caused by a radiotransparent cervico-facial foreign body intraorbital arteriovenous fistula secondary to penetrating injury. Arch Pediatr 2006; 13: 1264. |
| [4] | Cadwel JA. Post-traumatic thrombosis of internal carotid artery. Am J Surg 1936; 32: 523-52. |
| [5] | Choy AT, Gluckman PG, Tong MC, Van HC. Flexible nasopharyngoscopy for fish bone removal from the pharynx. J Laryngol Otol 1992; 106: 709-11. |
| [6] | Wadie GM, Konefal SH, Dias MA, McLaughlin MR. Cervical spondylodiscitis from an ingested pin: a case report. J Pediatr Surg 2005; 40: 593-6. |
| [7] | Allotey J, Duncan H, Williams H. Mediastinitis and retropharyngeal abscess following delayed diagnosis of glass ingestion. Emerg Med J 2006; 23: e12. |
| [8] | Yii NW, Quinn SJ, Andersson LC, Niranjan NS, Kenyon GS. Cervical necrotising fasciitis with pharyngeal perforation: treatment and reconstruction. Br J Plast Surg 1996; 49: 237-41. |
| [9] | Singh B, KantuM, Har EG, Lucente FE. Complications associated with 327 foreign bodies of the pharynx, larynx, and esophagus. Ann Otol Rhinol Laryngol 1997; 106: 301-4. |
| [10] | Smyth DA, Fenton J, Timon C, Mcshane DP. Occult pharyngeal perforation secondary to ’pencil injury’. J Laryngol Otol 1996; 110: 901-3. |
| [11] | Soroudi A, Shipp HE, Stepanski BM, Ray LU, Murrin PA, Chan TC, et al. Adult foreign body airway obstruction in the prehospital setting. Prehosp Emerg Care 2007; 11: 25-9. |
| [12] | Rouillon I, Charrier JB, Devictor D, Portier F, Lebret IK, Attal P, et al. Lower respiratory tract foreign bodies: a retrospective review of morbidity, mortality and first aid management. Int J Pediatr Otorhinolaryngol 2006; 70: 1949-55. |
| [13] | Jones NS, Lannigan FJ, Salama NY. Foreign bodies in the throat: a prospective study of 388 cases. J Laryngol Otol 1991; 105: 104-8. |
| [14] | Kosaki H, Nakamura N, Toriyama Y. Penetrating injuries to theoropharynx. J Laryngol Otol 1992; 106: 813-6. |
| [15] | Radkowski D, McGill TJ, Healy GB, Jones DT. Penetrating trauma of the oropharynx in children. Laryngoscope 1993; 103: 991-4. |
| [16] | Legent L, Narc P, Beauvillain P. ORL pathologie cervico-faciale. Paris: Masson; 2003: 2635-Molard O, Beauvilain de Montreuil C. Corps étrangers et perforation du pharynx. Encyclopédie médicochirurgicale (Elsevier, Paris). OtoRhino-Laryngologie, 20-620-A-10, 1998, 3p. |
| [17] | Malard O., Wagner R., Beauvillain de Montreuil C. Corps étrangers et perforation du pharynx. EMC (Elsevier Masson SAS, Paris), Oto-rhino-laryngologie, 20-620-A-10, 2008. |
APA Style
Wahab, H. A., Aminata, F., Harouna, S., Oumou, C., Mahamadou, D., et al. (2024). Foreign Body Trapped in the Oropharynx Requiring Emergency Tonsillectomy in a Case at Nianankoro Fomba Hospital in Ségou. International Journal of Otorhinolaryngology, 10(2), 54-57. https://doi.org/10.11648/j.ijo.20241002.12
ACS Style
Wahab, H. A.; Aminata, F.; Harouna, S.; Oumou, C.; Mahamadou, D., et al. Foreign Body Trapped in the Oropharynx Requiring Emergency Tonsillectomy in a Case at Nianankoro Fomba Hospital in Ségou. Int. J. Otorhinolaryngol. 2024, 10(2), 54-57. doi: 10.11648/j.ijo.20241002.12
@article{10.11648/j.ijo.20241002.12,
author = {Haidara Abdoul Wahab and Fofana Aminata and Sanogo Harouna and Coulbaly Oumou and Doumbia Mahamadou and Coulibaly Demba and Mohamed Saydi Ag Mohamed Elmehdi Elansari and Traore Bagouma and Dembele Ali and Amadou Coulibaly and Sanogo Boubacar and Mariam Sangare and Kone Fatogoma Issa and Boubacary Guindo and Siaka Soumaoro and Kadiatou Singare and Mohamed Aamdou Keita},
title = {Foreign Body Trapped in the Oropharynx Requiring Emergency Tonsillectomy in a Case at Nianankoro Fomba Hospital in Ségou
},
journal = {International Journal of Otorhinolaryngology},
volume = {10},
number = {2},
pages = {54-57},
doi = {10.11648/j.ijo.20241002.12},
url = {https://doi.org/10.11648/j.ijo.20241002.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20241002.12},
abstract = {Introduction: Pharyngeal foreign bodies, particularly in oropharyngeal locations, should raise concerns about the presence of an associated wound. They constitute a common pathology. Their diagnosis is most often easy, but difficult in the case of an unknown foreign body. We report a foreign body embedded in the lateral wall of the oropharynx which required emergency tonsillectomy. Observation: This is a 6-year-old child received urgently at the Nianankoro Fomba Hospital in Ségou 6 hours after the introduction of the foreign body (wheel spoke) into the tonsillar compartment. On admission to the ENT and head and neck surgery department, the child's general condition was poor, consciousness remained and the conjunctivas were normal-colored. On oropharyngeal examination, we note a sharp metallic foreign body measuring 30 cm and 2 mm in diameter located at the level of the posterior fold of the right amygdala. Furthermore, there is hypersialorrhea with blood streaking. Faced with the failure of an extraction attempt; we decided to take him to the operating room after a minimum assessment. The immediate postoperative course was unremarkable. The evolution was very favorable on the 10th day of the intervention. Conclusion: Pharyngeal foreign bodies constitute a vital emergency due to their appearance or location. Their management requires rapid intervention with suitable equipment. Prevention remains the best solution.
},
year = {2024}
}
TY - JOUR T1 - Foreign Body Trapped in the Oropharynx Requiring Emergency Tonsillectomy in a Case at Nianankoro Fomba Hospital in Ségou AU - Haidara Abdoul Wahab AU - Fofana Aminata AU - Sanogo Harouna AU - Coulbaly Oumou AU - Doumbia Mahamadou AU - Coulibaly Demba AU - Mohamed Saydi Ag Mohamed Elmehdi Elansari AU - Traore Bagouma AU - Dembele Ali AU - Amadou Coulibaly AU - Sanogo Boubacar AU - Mariam Sangare AU - Kone Fatogoma Issa AU - Boubacary Guindo AU - Siaka Soumaoro AU - Kadiatou Singare AU - Mohamed Aamdou Keita Y1 - 2024/09/23 PY - 2024 N1 - https://doi.org/10.11648/j.ijo.20241002.12 DO - 10.11648/j.ijo.20241002.12 T2 - International Journal of Otorhinolaryngology JF - International Journal of Otorhinolaryngology JO - International Journal of Otorhinolaryngology SP - 54 EP - 57 PB - Science Publishing Group SN - 2472-2413 UR - https://doi.org/10.11648/j.ijo.20241002.12 AB - Introduction: Pharyngeal foreign bodies, particularly in oropharyngeal locations, should raise concerns about the presence of an associated wound. They constitute a common pathology. Their diagnosis is most often easy, but difficult in the case of an unknown foreign body. We report a foreign body embedded in the lateral wall of the oropharynx which required emergency tonsillectomy. Observation: This is a 6-year-old child received urgently at the Nianankoro Fomba Hospital in Ségou 6 hours after the introduction of the foreign body (wheel spoke) into the tonsillar compartment. On admission to the ENT and head and neck surgery department, the child's general condition was poor, consciousness remained and the conjunctivas were normal-colored. On oropharyngeal examination, we note a sharp metallic foreign body measuring 30 cm and 2 mm in diameter located at the level of the posterior fold of the right amygdala. Furthermore, there is hypersialorrhea with blood streaking. Faced with the failure of an extraction attempt; we decided to take him to the operating room after a minimum assessment. The immediate postoperative course was unremarkable. The evolution was very favorable on the 10th day of the intervention. Conclusion: Pharyngeal foreign bodies constitute a vital emergency due to their appearance or location. Their management requires rapid intervention with suitable equipment. Prevention remains the best solution. VL - 10 IS - 2 ER -
ENT and Head and Neck Surgery Department, Nianankoro Fomba Hospital, Ségou, Mali