Introduction: jugulocarotid trauma is rare and serious. They can be immediately life-threatening due to the impact of serious hemorrhage or obstruction of the upper airways. Objective: The objective of this work is to describe the clinical and therapeutic aspects of these lesions. Observations: The time taken to treat our patients was less than 12 hours in all our patients. A pressure dressing was placed in two patients. All our patients benefited from a preoperative assessment with Rh grouping and possibly a blood transfusion as needed. Exploratory cervicotomy was performed in all patients with, as appropriate, repair or ligation of the internal jugular vein and suture of the carotid wounds. All patients received antithrombotic treatment, antibiotic prophylaxis and analgesic treatment at the end of the procedure. The postoperative course was simple in all cases. Conclusion: vascular wounds of the neck constitute an emergency. Prehospital care is an essential step in the management of these lesions. Faced with massive hemorrhage, only immediate surgical exploration associated with resuscitation measures determines the survival of patients. In other cases, an imaging assessment may be necessary in stable patients.
| Published in | International Journal of Otorhinolaryngology (Volume 10, Issue 1) |
| DOI | 10.11648/j.ijo.20241001.19 |
| Page(s) | 45-49 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Jugulocarotid Trauma, Emergency, Exploratory Cervicotomy
C | Cervical Vertebra |
| [1] | J. F. QUINOT, E. KAISER. Urgence devant une plaie cervicale [Emergency in front of a cervical wound]. EMC-Médecine 1. 2004, 157–164. |
| [2] | KONÉ FI, KEITA MA, SOUMAHORO S, KONATÉ N, DIARRA K. Historical Case of Cervical Penetrating Wound: From First Aid to Surgical Intervention. Hindawi Case Reports in Otolaryngology. 2017. 3p. |
| [3] | CESARE E, DRAOUA S, LEFORT H, TAZAROURTE K. Plaies pénétrantes du cou. [Penetrating areas of the neck.] SAMU de France urgence 2012. |
| [4] | BALLIVET DE REGLOIX S, CRAMBERT A, MAURIN O, PONS Y, BONFORT G, CLEMENT P. Plaies cervicofaciales par projectiles [Head and neck games using projectiles]. EMC - Oto-rhino-laryngologie 2016; 11(2): 1-11 [Article 20-860-B-10]. |
| [5] | INABA K, MUNERA F, MCKENNEY, MG. The nonoperative management of penetrating internal jugular vein injury. J Vasc Surg 2006; 43: 77-80. |
| [6] | Varghese A. Penetrating Neck Injury: A Case Report and Review of Management Indian J Surg 2013, 75(1): 43–46. |
| [7] | ALTABAA K, FIORETTI E, VERILLAUD B. Prise en charge des plaies cervicales avec atteinte vasculaire. À propos de 30 cas [Management of cervical wounds with vascular involvement. About 30 cases]. In Annales Françaises d’ORL et de pathologie cervicofaciale. Paris 2013. 130(4): A53 https://doi.org/10.1016/J.aforl. 2013.06.138 |
| [8] | VAUDEY JG. Plaies et ligature de la veine jugulaire interne [Games and ligation of the internal jugular vein]. In Vaisseaux sanguins—Maladie. Paris 1890. 60 P. |
| [9] | L. MARTIN. Traumatisme fermé des vaisseaux du cou [Trauma of closed vessels of the neck]. Prise en charge d’un polytraumatisé. Mapar 2002. 565-567. |
| [10] | Mahmoodie M, Sanei B, Moazeni Bistgani M, Namgar M. Penetrating Neck Trauma: Review of 192 Cases. Arch Trauma Res. 2012 1(1): 4. |
APA Style
Konaté, N., Nderagakura, S., Diarra, K., Sanogo, H., Guindo, B., et al. (2024). Jugulocarotid Trauma in Civil Practice: About Three (3) Cases. International Journal of Otorhinolaryngology, 10(1), 45-49. https://doi.org/10.11648/j.ijo.20241001.19
ACS Style
Konaté, N.; Nderagakura, S.; Diarra, K.; Sanogo, H.; Guindo, B., et al. Jugulocarotid Trauma in Civil Practice: About Three (3) Cases. Int. J. Otorhinolaryngol. 2024, 10(1), 45-49. doi: 10.11648/j.ijo.20241001.19
@article{10.11648/j.ijo.20241001.19,
author = {N’faly Konaté and Sixte Nderagakura and Kassim Diarra and Harouna Sanogo and Boubakary Guindo and Mohamed Ag El Ansari and Fatogoma Issa Kone and Naouma Cissé and Kalifa Coulibaly and Siaka Soumaoro and Kadiatou Sinkare and Ibrahima Bouare and Mohamed Keïta},
title = {Jugulocarotid Trauma in Civil Practice: About Three (3) Cases
},
journal = {International Journal of Otorhinolaryngology},
volume = {10},
number = {1},
pages = {45-49},
doi = {10.11648/j.ijo.20241001.19},
url = {https://doi.org/10.11648/j.ijo.20241001.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20241001.19},
abstract = {Introduction: jugulocarotid trauma is rare and serious. They can be immediately life-threatening due to the impact of serious hemorrhage or obstruction of the upper airways. Objective: The objective of this work is to describe the clinical and therapeutic aspects of these lesions. Observations: The time taken to treat our patients was less than 12 hours in all our patients. A pressure dressing was placed in two patients. All our patients benefited from a preoperative assessment with Rh grouping and possibly a blood transfusion as needed. Exploratory cervicotomy was performed in all patients with, as appropriate, repair or ligation of the internal jugular vein and suture of the carotid wounds. All patients received antithrombotic treatment, antibiotic prophylaxis and analgesic treatment at the end of the procedure. The postoperative course was simple in all cases. Conclusion: vascular wounds of the neck constitute an emergency. Prehospital care is an essential step in the management of these lesions. Faced with massive hemorrhage, only immediate surgical exploration associated with resuscitation measures determines the survival of patients. In other cases, an imaging assessment may be necessary in stable patients.
},
year = {2024}
}
TY - JOUR T1 - Jugulocarotid Trauma in Civil Practice: About Three (3) Cases AU - N’faly Konaté AU - Sixte Nderagakura AU - Kassim Diarra AU - Harouna Sanogo AU - Boubakary Guindo AU - Mohamed Ag El Ansari AU - Fatogoma Issa Kone AU - Naouma Cissé AU - Kalifa Coulibaly AU - Siaka Soumaoro AU - Kadiatou Sinkare AU - Ibrahima Bouare AU - Mohamed Keïta Y1 - 2024/06/19 PY - 2024 N1 - https://doi.org/10.11648/j.ijo.20241001.19 DO - 10.11648/j.ijo.20241001.19 T2 - International Journal of Otorhinolaryngology JF - International Journal of Otorhinolaryngology JO - International Journal of Otorhinolaryngology SP - 45 EP - 49 PB - Science Publishing Group SN - 2472-2413 UR - https://doi.org/10.11648/j.ijo.20241001.19 AB - Introduction: jugulocarotid trauma is rare and serious. They can be immediately life-threatening due to the impact of serious hemorrhage or obstruction of the upper airways. Objective: The objective of this work is to describe the clinical and therapeutic aspects of these lesions. Observations: The time taken to treat our patients was less than 12 hours in all our patients. A pressure dressing was placed in two patients. All our patients benefited from a preoperative assessment with Rh grouping and possibly a blood transfusion as needed. Exploratory cervicotomy was performed in all patients with, as appropriate, repair or ligation of the internal jugular vein and suture of the carotid wounds. All patients received antithrombotic treatment, antibiotic prophylaxis and analgesic treatment at the end of the procedure. The postoperative course was simple in all cases. Conclusion: vascular wounds of the neck constitute an emergency. Prehospital care is an essential step in the management of these lesions. Faced with massive hemorrhage, only immediate surgical exploration associated with resuscitation measures determines the survival of patients. In other cases, an imaging assessment may be necessary in stable patients. VL - 10 IS - 1 ER -
ENT and Head and Neck Surgery Department, University Hospital Center “Gabriel Touré”, Bamako, Mali
ENT and Head and Neck Surgery Department, University Hospital Center “Kamenge”, Bujumbura, Burundi
ENT and Head and Neck Surgery Department, University Hospital Center “Gabriel Touré”, Bamako, Mali
ENT and Head and Neck Surgery Department, Commune VI Reference Health Center, Bamako, Mali
ENT and Head and Neck Surgery Department, University Hospital Center “Gabriel Touré”, Bamako, Mali

Figure 1. Projectile entry port.

Figure 2. Cervical x-ray highlighted the projectile in the form of metallic hypodensity next to C4-C5.

Figure 3. Dissection and clamping of the internal jugular vein.
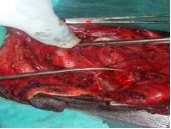
Figure 4. Reconstitution of the internal jugular vein.

Figure 5. Visualization of the carotid bifurcation gap.

Figure 6. carotid suture with prolène 4.0.

